ARMC welcomes RevPoint medical point-of-sale software. We see point-of-sale software everywhere else, so why not at hospitals? There’s a few things about this that I like, and a couple of things I don’t. Well, nothing’s perfect, and hospitals, just like any other business entity, need to get paid for the services they offer, since they have expenses, direct and indirect, and profit, even if they are a non-profit entity, since profits allow for growth, new services, and better equipment and training. This need to get paid makes them identical to every other business on the face of the planet. Even government entities need to collect the monies due them, whether it’s fees for services, taxes, grants, or budget infusions from their larger government parent entity. Nothing is free, except unwanted advice, and it is frequently worth what you had to pay for it. More on this later.
First, back to my $10.87 co-pay x-ray. Just a few short years ago, I waited until the radiology technicians at ARMC to developed the x-ray film, then carried my entire file over the Uroman’s office for him to compare the latest x-ray with the previous one, identifying the changes and the need for treatment. But this is no more, since the hospitals have all gone to digital photography, too. It is likely that only small doctor’s offices and chiropractors still use film, but they are glad to get the old equipment that others don’t want, which may be a significant improvement over what they currently have, for who wants an old, leaky x-ray machine? Eventually, digital x-ray machines will be as ubiquitous as digital cameras, since everyone has a camera, and a pretty good one, on their phone. The image of my stone and its current location were sent directly to Uroman’s office. He had reviewed it prior to my appointment. He blew into the examination room like a small tornado.
“In a hurry?” I asked.
Perplexed, he asked back, “What do you mean?”
“You came in here like you were rushing to put the fire out, as if I had spontaneously combusted or something,” I replied.
“Oh! Sorry. I just get so focused on what I’m doing I always seem to be in a hurry. I’m not, really,” he said.
“Then calm down.”
With that, he had a seat on the stool and rolled over next to the chair I was seated in. “Bad news. The stone has moved less than a centimeter since you were at the ER last week. It’s either gonna pass mighty slow, or it’s not going any further. Has it been causing you any pain?” he asked.
“Yes, but not nearly as much as it could. I can tell when it is moving. I get sharp sticks of pain when it moves a micrometer, but if was moving in earnest, I would’ve been back to the hospital. I’d have called you,” I said.
“You can wait it out, or we can blast it. It’s your call. We can go through this for several weeks, then blast it, or we can blast it now. Of course, you could pass it in the next fifteen minutes, but that is unlikely. What we can’t do, and you know this, is keep you pumped up on dilaudid for several weeks since that comes with its own set of problems.” I had already thought of that. The dilaudid was certainly keeping me comfortable, but it was interfering with my work as much as the stone, and I was already at the limit of a human’s ability to use it effectively without the risk of increasing tolerance. I didn’t want that. Neither did Uroman.
“Let’s blast it,” I said, forcefully, decidedly, without waiver.
“OK. That’s what I’d do, too. It’s a good choice. The good news is that there are no other stones present anywhere. When we get this one, it’ll be the last one. That doesn’t mean more won’t develop, but for the first time in several years you will be completely stone-free.”
“The last time I had lithotripsy, I received a bill from a third party, a certain Lithotripters of Mississippi, LLC, who was not in my PPO network. They were invisible to me. I had no way of knowing that this was going to happen. So who will I get the bill from this time? Who do you use for the lithotripsy?” I asked.
“I don’t know who it is. I mean, I know the technicians by name, but not the company information. You can get that at the hospital when you preregister,” he said, writing on a ARMC preadmission form and advising me to go over there to preregister as soon as possible, but no later than Friday morning, for the procedures which had been scheduled for 6:30AM on Monday 5/5/14.
“Now wait a minute. You see and deal with the lithotripsy truck and its technicians twice a week, and you don’t know the name of the company or where their corporate office is? I find that hard to believe,” I said. He was a bit peeved, but not too much.
“I can’t think of it right now. It is Lithotripters of Mississippi, but that is not their corporate parent’s name. I think they use different names depending on which hospital they work at. It’s confusing to me, too,” he said.
I knew I’d get this figured out just as soon as I got over to admissions. There we’d be again…me and those clerks. Me with lots of questions and them telling me they were just clerks and could not answer my questions. I’d have to find someone to give me the straight scoop, and I would, too. I shook Uroman’s hand. We agreed we’d see each other on Monday morning at 6:30. I was ready for relief. I had work to do but no wherewithal to do it, or even safely drive a car.
- The whole time I am doing this I am thinking of our men working in Louisville. I am thinking of my friend, Wilson, who lost his own home in the tornado but has no time to deal with that because he is trying to get his electrical distribution system rebuilt so his customers can have power…at least those with homes left to attach power to; some home sites, many home sites, are now just vacant lots except for the twisted metal and ripped up trees.
I leave Uroman’s office and go back to the hospital (ARMC). I tell the admissions receptionist that I am back, aren’t they glad, and hand her my precertification papers. She smiles and turns and goes back into the inner sanctum. I strain to hear the conversations that are going on, which no doubt consist of, “Who wants him this time?” with apparently no takers. Finally, the same young lady I had for the x-ray admission comes out and calls for me to come back to her cubicle. She has a smile on her face, but it looks a bit strained to me. I can’t say as I blame her.
I sat in the chair across from her in her cubicle and she asked me, in her sweetest voice, “Now, Mr. Sharp, what can we do for you this time?”
“I’m here to preregister for a lithotripsy on Monday,” I said, handing her the papers Uroman had given me. She does not ask me have I been there before. I am surprised by this. But she does ask for my ID and my insurance card, which I already have out and hand to her immediately upon her request. She starts entering the information all over again for yet another account. She calls the preadmissions number on my Cigna card, speaks to the clerk on the other end, finds out my deductible, reconfirms my co-pay, and learns what my maximum out of pocket costs will be. Having had a lithotripsy before, I already know pretty much what this will cost, and in one fell swoop will put me at my annual maximum out of pocket expense.
As she finishes entering the information, she prints out a document, looks at it, turns red in the face and lowers her eyes. I try to help her out here. “You’re afraid to tell me what it says on that piece of paper aren’t you?” I asked. She nodded her head. “Just slide it over here and let me look at it.” She reluctantly slides it over towards me, and though difficult for her, showing it to me is apparently easier than saying it out loud. I look at the paper. It says I will owe the hospital $1,400 up front in order to get the lithotripsy. I smiled when I saw this. I thought it would say $2,000. I told her so, and she seemed immensely relieved that there would be no awkward protests of hospital robbery, no personal vilification of her, the “just a clerk” doing her job, no bad feelings . . . nope, none of that.
She was speaking to me as I peered intently at the paper she had given me. She was speaking but I was not listening. I was livid over what I saw on the paper, which was plainly not her doing, but some code in the RevPoint program. ARMC has installed this health-care retail point-of-sale system, and I applaud this, because for the first time ever hospitals can give you an estimation of what your charges are likely to be. If we could shop for medical services like we shop for a new washing machine, we’d likely be surprised at the prices we could negotiate. With this new system, ARMC and RevPoint medical retail point-of-sale can take the codes (the proprietary American Medical Association Procedure Codes) input by the clerk from the description of the procedure the doctor listed on the preadmissions form and voila!….there appears your estimated charges. I later went to RevPoint’s web page to learn more about them. You can, too, right HERE.
RevPoint’s primary goal is to help medical facilities increase collections. Of course, their website touts its simple admissions process, it matching of patients with their likely PPO discounted price for the procedure, and smooth, seamless admissions, collections, and discharge processes. I can’t fault anyone for wanting to collect the money that is due to them for services they provide which I purchase, and I think it is good that there is finally some way to at least forewarn people what their charges might be, though the estimated charges are not necessarily the actual charges, which may be completely different and I expect one will still owe more money than their estimate, simply because they can and likely will charge more.
I have friends who are health care professionals who routinely say that all they ever get is the insurance money…that their patients hardly ever pay their co-pay. If you think being a doctor is all about raking in the money, just remember that money is how the nurses, receptionists, janitors, rent, insurance, and materials vendors are all paid. The same folks who think that all the money doctors take in is free for their personal discretionary spending…well those are the same folks who are liable to think that every dollar that goes into Bubba’s Bait Shop’s cash register is for the personal amusement of Bubba. Bubba needs to remember that he has to buy worms, crickets, and minnows or he soon will have no bait to sell, and with nothing to sell, no money goes in the cash register. He’ll be pawning that cash register before you know it to make a payment on his four wheel drive truck with the 18” lift kit and 24” tires.
Hospitals want to make their cash register ring, too. In addition to folks like me who can and will pay, there are those who can’t and won’t, and those who can and don’t. If I had debts, the hospital would certainly be the last one on my list to pay, since they are prohibited by law from charging interest on unpaid balances. If the choice is between the MasterCard charging me 23.675% APR and the hospital charging me 0%, well, what person in their right mind would pay the hospital first? Hospitals know this. They have been around a long time…even longer than MasterCard. Their best chance of getting their money comes when they can get it up front. RevPoint knows this, too. The have a nefarious little segment on their form, and this form was meant to be used for a screen script, I think, and not to be handed the patient. It is shown in the photo below.
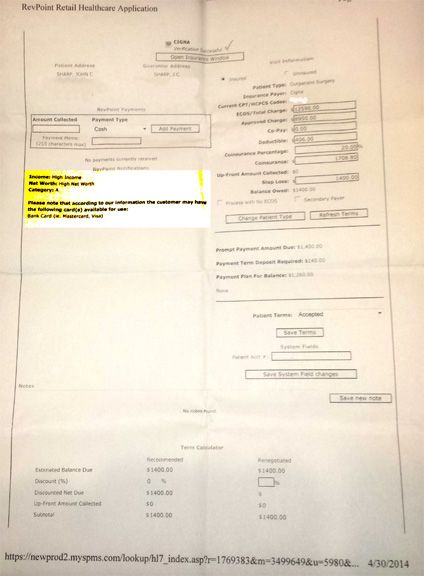
RevPoint has somewhere obtained information that my income is high and that I have a high net worth. Now, where do you suppose they would get this information? Their website says that they take this from demographics, but the demographics of rural Mississippi do not place me in high income and high net worth. It is more likely they would surmise that my income is low and that I have a negative net worth. Do you suppose they pulled a credit report from one of the credit reporting agencies? If so, did RevPoint just pull one on me? Do they have a deal with the credit reporting agencies to furnish limited information? Do they use the same sort of demographic lists that are used to send you free credit card offers? Are they making me pay up front simply because they think, because of the RevPoint system’s reporting, that I can? If that is true, then are they denying health-care to those who have insurance but cannot afford to pay they co-pays and deductibles up front?
This, I think, is a sneaky bit of business. I expect they will hear from me.
Is all health-care information now linked to insurance, income, lifestyle, family history, genetics, education….in other words, will all of my relevant information be accessible to clerks at the hospital every time I need two stitches because of an accident with a kitchen knife? Remember, this is the same clerk who would not take my word for it that I have been there before, but now she thinks she may have some understanding of my financial situation.
Does it say how I take my coffee, I wonder?
Enough of RevPoint. I understand the results it promises to its customers: collect more money. In my capitalist heart, I don’t have a problem with that. I have a problem with something that is so awkward that their own trained clerks are ashamed and afraid to use it. ARMC should have a management person available at all times to be able to intervene on behalf of the clerks, who clearly don’t like the scapegoat status this system inflicts on them…and for that matter, neither do I.
It is not for my advantage, even though the web site says it offers me advantages, too. The only one I can detect is that I have some idea, going in, on how much the service is likely to cost me. I’m sure the RevPoint service leaves a lot of things out. Remember, its main, stated goal is to help hospitals collect more money.
The admissions clerk and I got through all those things and were at the point where she was happy that I was not going to complain about the $1,400 up front co-pay cost. She said, “I’ll just need to collect the $1,400 and we can get you all set up.”
“No, ma’am. This is Wednesday. The lithotripsy is not scheduled until Monday. I may pass that stone between now and then and not even need the lithotripsy, so will just wait until Monday to pay you the $1,400,” I said, thinking this was a reasonable thing to do.
“But I need to collect this today,” she protested, but kindly so.
“No, ma’am. I will not pay it today. I’ll bring it with me on Monday morning,” I said. She nodded her head, and then I said, “There is just one more thing I need.” I could see it in her eyes, that look of the mouse just as it bites the cheese on the trap and hears the sound of a metallic transient….the big uh-oh, here it comes look. She braced herself.
“The last time I had a lithotripsy done, I received a bill from a third party called Lithotripters of Mississippi, which is subsidiary of Lithotripters, Inc., of Dallas, Texas. They were not part of my PPO network and it cost me a lot of extra money. This third party arrangement was unknown to me, so I need to know who will be sending me the actual bill for the lithotripsy,” I said.
“We do it here,” she replied, “So you will get the bill from the hospital.”
“I don’t think so. You don’t have your own lithotripsy machine here. The truck comes in to ARMC on Monday and goes to that other hospital in town on Wednesday. The lithotripsy folks provide their own billing. I need to know who it is so I can confirm their PPO status with my insurance, or negotiate something with them if they are out-of-network.”
Explaining this caused us both no end of confusion. She was doing the best she could, but I was just not a typical patient. I had questions and I demanded answers to them. The concept of third-party billing was completely foreign to her understanding. I failed to get it across. She made phone calls to people who referred her to other people, and someone finally told her that Uroman was the one I needed to ask. When she told me that, she just beamed, thinking she had finally found the answer that I needed.
“I asked Uroman, He said that he didn’t know, that you would be able to tell me. Someone, if not in admissions, then in billing, or in insurance, or in administration knows who this entity is. I need to know, too,” I said. I had to define the word entity to her. She made more phone calls. She got lots of voice mails. Two or three more senior admissions clerks came over and tried to help, mostly by trying to explain to me that I was wrong about what I already knew. I didn’t budge. She finally got hold of someone in billing with some authority and began trying to explain what it was that I was asking for. She was not doing well since she did not understand herself.
She was told that the person I needed to talk to was in an important meeting. I told her to tell them that an important customer was needing an answer to an important question and someone needed to go and get someone out of that important meeting. Someone did. The clerk put the person thus interrupted from the important meeting on the phone with me, the important customer. She knew exactly what I needed and who I needed to talk to. She offered to transfer me immediately to a certain man named Morty.
“NoNoNo!” I said, “Give me his full name and phone number first, then transfer me, please.”
I was then transferred to Morty Morty. After a few rings, I got his voice mail. “This is Morty Morty,” the recording of his voice stated, “I am currently away from my desk. Please leave your name and number at the tone and I will return your call as soon as possible.” I was not impressed, or at all confident that I would get a return phone call anytime soon, but I left the message, briefly telling Morty what I needed, not just giving him my name and my number. With that, there was nothing left to do but finish one more bit of paperwork.
The clerk slid that piece of paper across the desk asking me to sign it, acknowledging that sometimes the hospital used anesthesiologists who would send me a separate bill that was not covered under the hospital’s bill. In other words, I might get a third party bill. I had just spent thirty minutes trying to explain to her what a third-party bill was and she never got it, even though she was familiar with third-party anesthesiologists. Apparently she only thought this applied to what she had been trained to apply it to. I admit that this was not all her fault. She needed more training and support from her supervisors, who all, mysteriously, seemed to be in important meetings. It must have been the same meeting they were all in a couple of hours earlier when I was there to get my x-ray. Maybe they were meeting about me, and discussing how they needed to spend more time training their employees to deal with difficult patients. Maybe they were meeting about empowering employees to make decisions. Maybe they were meeting about keeping more power for themselves and letting their employees be less responsible while simultaneously making themselves more inaccessible by planning more meetings. Never underestimate the inefficiency of a large organization, and this one is remarkably inefficient.
They were even inefficient in collecting the $1,400, as this was their goal with their RevPoint system and they failed to achieve it, and failed completely.
- Through all of this, I thought of our men working from can to can’t, and all the people in Louisville who didn’t even have a hospital to go to anymore since the tornado had damaged theirs to the point of near ruin. I was thinking I should be working, not spending this time quibbling with hospital clerks and their invisible supervisors. I was thinking of the people who lost their lives and their loved ones and their homes in a single minute of terror. There was no consolation there.
I was then sent back to the preadmissions nurse. Remarkably she had overhead nearly all of our exchange. She slipped me a piece of paper with the name of Healthronics, Inc., Dallas, Texas. “They are the ones who provide the lithotripsy,” she said. “Call them. If they are out of your network and you can talk to them about how they will bill you. This happens all the time.”
“Why didn’t you speak up sooner?” I asked.
“I’ve tried before, but I am not allowed involve myself with admissions. I only interview patients for health information and to advise them of what to expect at same day surgery after they send them back here, but that’s what you are looking for,” she said.
It was, too. Bless her. It was one more marvel of inefficiency that one person seated so as to be able to have overheard the entire exchange and who had the exact information I was looking for was prohibited from telling me, or the clerks, what we all needed to know. She was an angel. “I’ve been around,” she said.
Little did I know it, but others were working on my behalf, too. Jane Doe was the one who had been interrupted from them meeting only to refer me to Morty Morty. Jane had taken up my case, perhaps after Morty had listened to my message and directed her, or perhaps on her own…I’ll never know, but I did get an official answer in a string of e-mails between Jane Doe from ARMC and June Apple from Lithotripters, LLC, a division of Healthtronics. Morty Morty was copied on the e-mails, so he may have precipitated them.
This is how they went:
From: Jane Doe<jdoe@ARMC.org>
To: June Apple <japple@lithotrpters.com
June, We have a patient, John C. Sharp that is scheduled for Lithotripsy on Monday, May 5th and his insurance is considered out of network if the billing is done by Healthtronics (MS Lithotripters). We need to bill this one. Please let me know if this will be OK.
His insurance is Cigna. Thanks for your help.
Jane Doe Accounting ARMC
—————————–
From: June Apple <japple@lithotrpters.com
To: Jane Doe <jdoe@ARMC.org>
Hi, June. I can’t find this patient in our system. Do you have a DOB?
——————————
From: Jane Doe<jdoe@ARMC.org>
To: June Apple <japple@lithotrpters.com
It’s 7/4/57 Thanks!
——————————
From: June Apple <japple@lithotrpters.com
To: Jane Doe <jdoe@ARMC.org>
Hmmm, I still can’t find this patient. But, I have notified our billing department that you all will bill it when they come across it to verify.
——————————
From: Jane Doe<jdoe@ARMC.org>
To: June Apple <japple@lithotrpters.com >
Thanks, June. I’ll let Mr. Sharp know.
Jane
——————————
From: Jane Doe <jdoe@ARMC.org>
To: missippichris@yahoo.com
cc: Morty Morty <mmorty@ARMC.org>
cc: June Apple <japple@lithotripters.com>
Mr. Sharp Per June Apple with MS Lithotripters they do not have you in the system yet. However, she is forwarding my request to their billing department letting them know that the hospital will be doing the billing for your procedure on Monday. I will follow up with her to make sure that the request was received.
Thanks!
Jane Doe
——————————————
To: Jane Doe <jdoe@ARMC.org>
From: missippichris@yahoo.com
Jane:
Thank you very much. Your extra effort on my behalf is sincerely appreciated.
John C. (Chris) Sharp
————————————–
From: Jane Doe <jdoe@ARMC.org>
To: missippichris@yahoo.com
It is my pleasure!
———————————–
There is help for the persistent (difficult). Though I have not yet received my bill, which will be the ultimate confirmation that things went as planned, people who make those decisions have agreed to do exactly what I have asked them to do, or at least made every effort to do so. But they would not have done so if I had not persisted.
So I left the hospital, my admission papers in my hand and everything all set for Monday morning at 6:30. I was to bring the money and all my medications. Later that day, I also received the return phone call from Morty Morty, who asked me had I gotten the issue squared away to my satisfaction. I thanked him for following up and confirmed that I seemed to get it all worked out.
I did not want to bring all my medications to the hospital, so I made a spreadsheet that showed them all, the dosages, and my prescribed times to take them. And before we left the house, I put fourteen one hundred dollar bills in an envelope and gave them to Debbie. I put on my most colorful sweats and tee-shirt, and off we went to the hospital. When I got to admissions, I showed them my papers and they escorted me straight back to same day surgery. No one tried to collect the $1,400. My nurse came in to my room and introduced herself, as did the anesthesiologist. They were running a bit behind schedule the nurse said, and the anesthesiologist, Dr. Amnesium, said they would be giving me Propofol, Fentanyl, and Lorazepam, which is all pretty potent stuff. Nurse Betty was to be my anesthetist, and Uroman came charging in and said they’d be taking me back just any minute.
I asked about the $1,400 and was told with shrugged shoulders that the business office was not yet open, so no one could receive the money. Ironically, in spite of the RevPoint system’s best intentions, I went in there owing $1,400, went in prepared to give them the entire $1,400, and no one was prepared to receive it. I left the hospital with the same fourteen one hundred dollar bills I went in there with. Of course, I’ll pay them, but not until after my insurance has done all of its PPO discounting, which will mean that I’ll still owe them the maximum out of pocket expense.
Now here’s something mean and low down for people to consider. If I were on the Magnolia Health Plan, which is the only plan offered in my area of Mississippi under the HealthCare.Gov exchange website, under their rules, if I go out of network, they will pay nothing. NOTHING. Now ARMC does not participate with Magnolia Health Plan, that other hospital in Meridian does. But if they did, and the patient receives a bill from an out of network facility, the patient is not covered, nor does the amount count towards any deductibles or maximum out of pocket costs. This is a dangerous thing. Patients must be diligent to explore all the various caregivers, health service providers, anesthesiologists, radiologists, and laboratory services who may be quite invisible to them who are not part of their network.
Perhaps the ACA should require full disclosure of all the invisible entities likely to be sending a bill to the patient for any reason.
I am through with this now. There may be a chapter 4, particularly if something goes wrong with my billing that you need to know about. My kidney stone has been blasted by Excoropreal Shock Wave Lithotripsy, reduced to sand grain size bits by acoustic waves of 60Hz to 120Hz. 60Hz is an audible wave that makes music sound muddy. 120Hz is an audible wave that gives the bass in music some thump. The 100 to 120 Hz waves are the audible waves that make you want to move with the music. Everyone likes them, but not everything. Kidney stones don’t like them at all.
And someone at ARMC is no doubt, right this very minute, planning a meeting to discuss what happened to the $1,400. All they need to do is call me. I’ve still got it in an envelope with their name on it. Their policy was to collect it. My policy was to pay it at the time the services were rendered, just like they asked me to. They should make sure that they have the capability of receiving it.
Never underestimate the inefficiency of large organizations.
- Small organizations? Well, Louisville Utilities is a small organization as far as electrical utilities go. And McElroy Electric? We are a small organization as far as utility electrical contractors go. But we are both efficient, have built a mile of power line a day since the great tornado. And all I had to suffer was a kidney stone. There’s lots of folks there who would gladly trade what they lost for a mere kidney stone.
All you patients out there…if you don’t take care of and be responsible for your business, who do you think is going to do it for you?
Who will be your advocate?
Note added 5/13/14……the description “sand grain size bits” was prematurely optimistic, I’m afraid. But it’s all history now.
©2014 Mississippi Chris Sharp
